INTRODUCTION
Suicide is a deliberate act leading to death, constituting one of the main causes of preventable mortality (World Health Organization [WHO], 2024). Every year it accounts for one million deaths worldwide, affecting both civilian and military populations, with military suicide rates sometimes surpassing those due to accidents or combat (Kuehn, 2009; Olfson et al., 2017; Nock et al., 2013; Naifeh et al., 2019).
Although U.S. military personnel historically had lower suicide rates than civilians, since 2008, these rates have exceeded those of the general population (Kuehn, 2009; Nock et al., 2013). A systematic review of 1,278,837 active-duty service members found an 11% prevalence of suicidal ideation (95% CI 10-13%) and an 11% prevalence of suicide attempts (95% CI 9-13%) (Moradi et al., 2021). The estimated suicide mortality rate in this group is 18.5 per 100,000 person-years, making it the second leading cause of death (Nock et al., 2013).
In Mexico, there is a dearth of research on military suicide risk. A study of 246 Mexican naval personnel at a mental health facility reported suicidal ideation in 24.39% and suicide attempts in 9.76 % in the past year. Risk factors included lower military rank, a family history of suicide, and depressive and personality disorders. Suicide attempts were more common among young, single personnel with fewer than four years of service (Ocampo-Ortega & Portillo-Wong, 2020).
Military personnel face unique stressors that increase their risk of sleep disorders, including irregular shifts, deployment stress, and frequent relocation (Taylor et al., 2016). Sleep disturbances are widespread among this population, with 48.6% experiencing poor sleep quality and 11% having a diagnosed sleep disorder, primarily insomnia and obstructive sleep apnea (Capaldi et al., 2019).
Insufficient sleep is linked to post-traumatic stress disorder, depression, anxiety, and traumatic brain injury (Suh et al., 2013; Mysliwiec et al., 2013). It is also a recognized independent risk factor for suicide (Pigeon et al., 2012; Ribeiro et al., 2012; Bernert et al., 2015; Woznica et al., 2015; Vargas et al., 2020). However, some researchers argue that suicide risk is secondary to depressive disorders, as insomnia is a symptom of depression (McCall & Black, 2013; Winsper & Tang, 2014).
Although the neurobiological mechanisms linking sleep deprivation to cognitive dysfunction are not yet fully understood, evidence suggests that sleep loss impairs prefrontal cortex function, affecting cognitive tasks dependent on this region (Demos et al., 2016). Since the prefrontal cortex regulates higher-order cognitive functions (Lowe, Safati & Hall, 2017), suboptimal activity during sleep restriction could explain observed deficits (Jones & Harrison, 2001).
This study seeks to examine the association between Pittsburgh Sleep Quality Index variables, depression, and suicidal ideation in the past month among Mexican naval personnel evaluated at the psychiatry service of the Hospital Naval de Especialidades de Veracruz (HOSNAVESVER).
METHOD
Study design
This observational, analytical, cross-sectional study was conducted at HOSNAVESVER between April 2020 and November 2021.
Participants
A non-probability sample of military naval personnel referred for psychiatric evaluation by their superiors participated in the study. Retired military personnel, military personnel who had been evaluated by another psychiatric specialist or had received specific treatment for a sleep disorder in the past month were excluded from the study. Military personnel with a diagnosis of schizophrenia, severe bipolar disorder (mania with psychotic symptoms), cognitive impairment due to any cause and military personnel with a recent history of severe head trauma were also excluded. During the study period, 275 military personnel underwent psychiatric evaluation, 59 of which (21.45 %) did not agree to participate in the study. No significant differences were observed in the variables of military personnel who did or did not agree to participate However, the proportion of military personnel belonging to the marine infantry who agreed to participate in the study was greater than that of other services (88.73% of marines versus 75% of military personnel from other services; χ² = 6.06; p = .014).
Measurements
A questionnaire on sociodemographic variables, the Pittsburgh Sleep Quality Index (PSQI) (Jiménez-Genchi et al., 2008) and a semi-structured psychiatric interview using the ICD-10 depressive disorder diagnostic criteria were administered. Suicidal ideation in the past month was assessed with the question from the suicidal risk section of the MINI Neuropsychiatric Interview version 5.0 (Lecrubier et al., 1997).
The ICD-10 criteria for depressive disorder require the presence of a set of core symptoms together with additional features determining the severity of the episode. Core symptoms include depressed mood, loss of interest and enjoyment and increased fatigability or reduced energy (at least two). In addition to core symptoms, (at least three, depending on the severity classification) of the following symptoms should be present: impaired concentration and attention, low self-esteem and feelings of worthlessness, ideas of guilt and self-reproach. Other symptoms include pessimistic views of the future, ideas or acts of self-harm or suicidal thoughts, disturbed sleep, and diminished appetite. Symptoms must have been present for at least two weeks and should cause significant distress or impairment in social, occupational, or other important areas of functioning (WHO, 2019).
The Pittsburgh Sleep Quality Index (PSQI) is a self-rated questionnaire assessing sleep quality and disturbances during a period of one month. Nineteen individual items are grouped together to obtain seven “component” scores: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleeping medication use, and daytime dysfunction. The sum of scores for these seven components yields a global score. Clinical and clinimetric properties of the PSQI were assessed over an 18-month period with “good” sleepers (healthy subjects, n = 52) and “poor” sleepers (depressed patients, n = 54; sleep-disorder patients, n = 62). A global PSQI score greater than 5 yielded a diagnostic sensitivity of 89.6% and a specificity of 86.5% (kappa = .75, p less than .001) in distinguishing between good and poor sleepers (Buysse et al, 1989). The PSQI has been translated into Spanish (Royuela & Macías, 1997).
In Mexico, a cross-sectional study was conducted to evaluate the reliability and factorial structure of the Spanish version of the PSQI in a sample of psychiatric patients and control subjects. The study showed acceptable reliability (Cronbach’s alpha = .78), significant correlations between the components and the global score (.53–.77), and a two-factor structure (sleep quality and sleep duration) (Jiménez-Genchi et al., 2008).
The suicidal risk section of the MINI Neuropsychiatric Interview version 5.0 is designed to quickly screen for the presence and severity of suicidal ideation and behaviors in the past month. The section begins with direct questions to determine whether the respondent has experienced thoughts related to death or self-harm. For example, it asks: “During the past month, have you thought that you would be better off dead, or have you wished you were dead?” “Have you wanted to harm yourself?” and “Have you thought about suicide?” These questions aim to capture a range of ideations—from passive thoughts about being dead to active suicidal thinking or a desire for self-harm. In this study, suicidal ideation was considered positive when an affirmative response was given to any of the three previous questions (Lecrubier et al., 1997).
Procedure
Patients referred for external psychiatric evaluation were invited to participate in the study. They were informed of the research and signed an informed consent form. Once the patient had agreed to participate, an interview was conducted. It included depressive symptoms based on the clinical criteria of the ICD-10 and questions about suicidal ideation from the MINI neuropsychiatric interview, after which the PSQI was administered. Evaluation time ranged from 30 to 40 minutes. Appropriate pharmacological treatment, psychological interventions and a safety plan were suggested for participants with depression and suicidal ideation, including hospitalization when necessary.
Statistical analysis
Variables were described in percentages and means. The chi-square test was used for the bivariate analysis and odds ratios were calculated with 95% confidence intervals. A p value less than .05 was considered significant. In the bivariate analysis, the association of the variables included in the PSQI and the presentation of suicidal ideation was analyzed using the chi-square test, calculating odds ratios and 95% confidence intervals. These variables included sleep latency, sleep duration, sleep efficiency, sleep disturbances such as difficulty falling asleep, waking up in the middle of the night or early morning, having to get up to use the bathroom, difficulty breathing, loud snoring, feeling hot or cold while sleeping, frequent nightmares, pain while sleeping, poor subjective sleep quality and daytime dysfunction (reduced daytime alertness, reduced daytime enthusiasm), and depressive disorder. PSQI variables such as difficulty falling asleep, waking up in the middle of the night or early morning, having to get up to use the bathroom, difficulty breathing, loud snoring, feeling hot or cold while sleeping, frequent nightmares, pain while sleeping, poor subjective sleep quality and reduced daytime alertness were considered positive if they had occurred three or more times a week during the past month. Poor subjective sleep quality was considered positive if the respondent answered “bad or very bad” in the past month. Reduced daytime enthusiasm was considered positive if their response was “a problem or a major problem” in the past month. Poor sleep quality was defined as a PSQI score over five. Finally, multivariate analysis was presented using logistic regression to determine the association between PSQI variables and suicidal ideation, with the inclusion of confounding variables such as age, sex and depression in the model. Data were analyzed using STATA 10.
Ethical considerations
The study was approved by the Bioethics Committee of the Universidad Cristobal Colón Campus Calazans in Boca del Río, Veracruz (Authorization Form No. 388). The study was based on the principles of the Helsinki Declaration and the Mexican General Health Research Act. Participants signed the informed consent letter on the understanding that refusal to participate in the study would not affect their subsequent medical or psychological care.
RESULTS
Sociodemographic and military characteristics of articipants
The total sample included 216 participants, 27.78 % of whom were female and 72.22 % male, with an average age of 33 years (SD 8.28, range 15-53 years). The average number of years in active service was 11.33 years (SD 7.55, range 0-29 years). Depressive disorders were present in 20.48 % of the sample (n = 43). At the time of the interview, 33.8 % (n = 73) of respondents had experienced suicidal ideation in the last month. (Table 1).
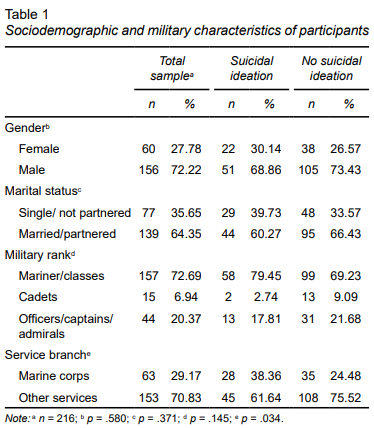
The prevalence of suicidal ideation was higher in men (68.86 %) than women (30.14%), although this difference was not statistically significant (p = .580). Regarding marital status, 35.65% were single or unpartnered, while 64.35% were married or partnered. No significant association was found between marital status and suicidal ideation (p = .371). Regarding military rank, most participants were sailors/petty officers (72.69 %), followed by officers/captains/admirals (20.37 %) and cadets (6.94%). Although suicidal ideation appeared to be more prevalent among sailors/petty officers(79.45 % vs. 69.23 % in those without ideation), this difference was not statistically significant (p = .145). Finally, as regards the branch of the Navy to which they belonged, 29.17 % of respondents belonged to the Marine Corps, and 70.83% to other services. A statistically significant association was found between suicidal ideation and belonging to a service other than the Marine Corps (p = .034), suggesting that members of these other services might be at a higher risk.
Association between sleep variables, depressive disorders, and suicidal ideation
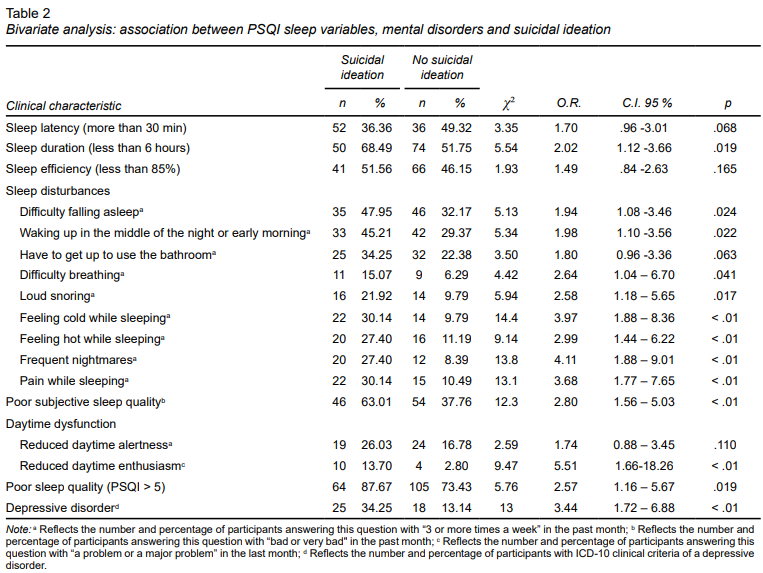
In regard to PSQI sleep variables, 78.24% of the sample met the criteria for poor sleep quality. Average sleep latency in the sample was 52.78 minutes (SD 68.86; range 0 - 420 minutes). The average number of reported hours of sleep per night was 5.2 hours (SD 1.93; range .5 - 11 hours), with 124 military personnel reporting sleeping fewer than six hours per night in the past month (57.4% of the sample). The mean sleep efficiency in the sample was 79.70% (SD 20.52; range 12.5 - 100%).
Table 2 presents the bivariate analysis of sleep variables in the PSQI and the presence of suicidal ideation. Military personnel with poor sleep quality had a 2.57 times greater risk of presenting suicidal ideation compared to military personnel with adequate sleep quality (p = .019). Several significant associations were found between sleep parameters and suicidal ideation: sleep duration < 6 hours (OR = 2.02, p = .019), difficulty falling asleep (OR = 1.94, p = .024), waking up in the middle of the night or early morning (OR = 1.98, p = .022), difficulty breathing (OR = 2.64, p = .041), loud snoring (OR = 2.58, p = .017), feeling cold while sleeping (OR = 3.97, p < .01), feeling hot while sleeping (OR = 2.99, p < .01), frequent nightmares (OR = 4.11, p < .01, pain while sleeping (OR = 3.68, p < .01), poor subjective sleep quality (OR = 2.80 (p < .01), and reduced daytime enthusiasm (OR = 5.51, p < .01). Since one exclusion criterion for participating in the study was having taken sleep medication in the past month, item 7 of the PSQI was omitted from the analysis. At the same time, the presence of a depressive disorder was closely linked to suicidal ideation (OR = 3.44, p < .01). These results indicate that poor sleep quality and depressive symptoms are key risk factors for suicidal ideation.
Adjusted logistic regression
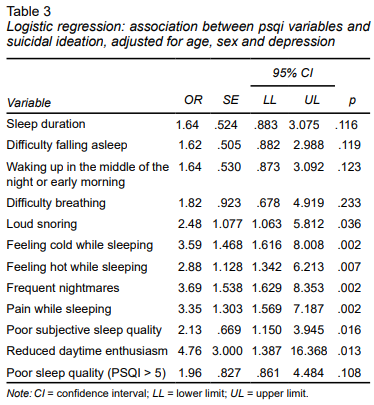
Logistic regression analysis, adjusted for age, sex, and depression, showed that certain sleep variables were significantly associated with suicidal ideation (Table 3): feeling cold while sleeping (OR = 3.59, p = .002), feeling hot while sleeping (OR = 2.88, p = .007), and loud snoring (OR = 2.48, p = .036). Other variables included frequent nightmares (OR = 3.69, p = .002), pain while sleeping (OR = 3.35, p = .002), poor subjective sleep quality (OR = 2.13, p = .016) and reduced daytime enthusiasm (OR = 4.76, p = .013). Variables such as sleep duration, difficulty falling asleep, waking up in the middle of the night or early morning, difficulty breathing and sleep quality were not significantly associated after adjusting for age, sex, and depression. These results reinforce the idea that specific sleep disturbances, particularly pain while sleeping, temperature dysregulation, nightmares, and reduced daytime enthusiasm, may be involved in suicidal ideation, even after adjusting for demographic variables and depression.
DISCUSSION AND CONCLUSION
This study is part of a research project based on a clinical sample of naval military personnel at risk of suicide. It highlights the strong association between sleep quality and suicidal ideation among the military personnel evaluated. A high prevalence of poor sleep and its correlation with depressive symptoms emphasize the need for targeted interventions to improve rest in this population. Multivariate analysis revealed that factors such as feeling cold or hot while sleeping, loud snoring, frequent nightmares, and reduced daytime enthusiasm remained significantly associated with suicidal ideation, even after adjusting for depression, age, and sex. This suggests that sleep problems may play an independent role in suicide risk rather than merely reflecting depressive symptomatology.
Military service members face a number of stressors and challenges putting them at a higher risk for insomnia than most civilians (Taylor et al. 2016). The observed percentage of poor sleep quality in this study (78.24% of the sample) is higher than that obtained in the study by Troxel et al., (Troxel, et al. 2015), who also used PSQI and found that 48.6% of a total sample of 1,957 military personnel experienced sleep problems. Although both studies address the impact of sleep disturbance on military personnel, they differ in scope, methodology, and focus. The U.S. study drew on a large, cross-sectional survey (N = 1,957) across all branches of the armed forces, analyzing the prevalence and consequences of sleep problems with a focus on operational readiness and mental health outcomes. Conversely, our study utilized a clinical, cross-sectional design with a smaller sample (N = 216) of naval personnel referred for psychiatric evaluation, specifically investigating the association between sleep quality and suicidal ideation using the Pittsburgh Sleep Quality Index (PSQI) and a psychiatric interview. Despite methodological differences, both studies identified high rates of sleep disturbances and highlighted shared risk factors such as nightmares, snoring, and sleep-related pain. However, our study found that specific sleep disruptions, including temperature-related awakenings, were independently associated with suicidal ideation, even after adjusting for depressive symptoms. Similar results regarding the association between sleep disorders and suicide risk have been reported in other studies (Ohayon, 2005; Taylor et al., 2007; Sjöström et al., 2007; Richardson et al., 2018; McCall & Black, 2013; Nadorff et al., 2013; Littlewood et al., 2019, Vargas et al., 2020).
In the present study, global sleep quality was not associated with the presence of suicidal ideation when depressive disorders were included in the logistic regression model. However, it was observed that factors such as feeling cold or hot while sleeping, loud snoring, frequent nightmares, and reduced daytime enthusiasm were independently associated with suicidal ideation. It is worth mentioning the possibility of the influence of environmental variables (excessive cold or heat) that affect the military population to a greater extent than other populations (Mysliwiec et al., 2016). Ribeiro et al. (2012) conducted a longitudinal study of U.S. military personnel, observing that insomnia predicted suicidal ideation even when controlling for depression, hopelessness, PTSD, anxiety, and substance abuse. Their results support the notion that sleep disturbances are independent risk factors for suicidality, reinforcing the importance of sleep-focused interventions in high-risk military groups. Although our study emphasized the predictive value of sleep disturbances beyond depressive symptoms, the longitudinal design of the study by Ribeiro et al. provides stronger evidence for a directional relationship between sleep problems and suicidal thoughts. Conversely, the detailed analysis of sleep parameters in our study offers valuable insights into specific sleep issues that may contribute to suicide risk. Together, these findings suggest that comprehensive sleep assessments should be incorporated into suicide prevention strategies in military settings and that future research should explore the underlying mechanisms linking sleep disturbances to suicidal behavior.
Decades of research have conclusively shown that adequate sleep quality supports cognitive abilities ranging from simple response speed to problem-solving, flexible thinking, and the ability to integrate new information into a common mental model. These mental processes underlie successful military operations (Seelig et al. 2010; Mysliwiec et al., 2016). Sleep is a vital military resource, hence the importance of having tools for the early, systematic detection of this health problem (Capaldi et al., 2019).
Sleep disruption is a particularly relevant problem among military personnel. Insomnia rates among military service members increase significantly (2.5-fold) during and after deployment to combat sites (Seelig et al. 2010) and may be associated with the high rates of suicidal ideation and attempted suicide observed in this population (Ribeiro et al. 2012; Leardmann et al., 2013). All the study variables associated with the presentation of suicidal ideation have a direct effect on nocturnal awakenings. Frequent nocturnal awakenings may be more distressing and produce greater dysfunction at the prefrontal level than other sleep continuity variables and better account for poor subjective sleep quality (Pigeon et al., 2012; Bernert et al., 2015; Woznica et al., 2015; Vargas et al., 2020).
Littlewood et al. published data from an ecological momentary assessment study suggesting that subjective sleep quality as well as objective and subjective short sleep duration significantly predicted suicidal ideation the following day (Littlewood et al., 2019). This study provides the first real-time examination of the relationship between sleep parameters, suicidal ideation, and entrapment. Findings revealed a unidirectional association, where shorter sleep duration and poorer sleep quality predicted increased suicidal ideation the following day, even after controlling for anxiety and depression. Additionally, sleep quality moderated the relationship between pre-sleep entrapment and suicidal ideation on awakening, suggesting that poor sleep increases the impact of emotional distress before sleep on next-day suicidal thoughts. Clinically, these findings highlight the importance of assessing and treating sleep disturbances in individuals at risk of suicide. Improving sleep duration and quality could serve as a potential intervention strategy to mitigate suicidal ideation. Psychological interventions targeting sleep problems, such as cognitive behavioral therapy for insomnia (CBT-I), could play a crucial role in suicide prevention efforts (Mysliwiec et al., 2016).
This study has notable strengths. First, it examines a high-risk population, providing valuable insights into the association between sleep quality and suicidal ideation among Mexican naval personnel—a group with unique occupational stressors. Second, the study employs validated assessment tools, including the Pittsburgh Sleep Quality Index (PSQI) and the MINI Neuropsychiatric Interview, ensuring reliable measurement of sleep disturbances and suicidal ideation. Third, the study adjusts for key confounding variables such as age, sex, and depression, allowing for a more accurate evaluation of the independent relationship between specific sleep disturbances and suicidal ideation. Moreover, the research highlights the importance of environmental factors such as extreme temperatures, nightmares, and snoring—factors often overlooked in suicide risk assessments. Finally, by focusing on an understudied military population, this study contributes to the growing body of evidence on sleep-related suicide risk, underscoring the need for tailored interventions in military mental health care.
This study also has limitations that should be considered when interpreting findings. First, the sample was limited to 216 naval personnel from a single psychiatric clinic, introducing selection bias and reducing the generalizability of results to the broader military population. It is necessary to include all military naval personnel at the national level, which could be done at the annual physical evaluation through the administration of self-applicable scales such as the PSQI used in the present study. Second, the cross-sectional design precludes establishing causality between sleep quality and suicidal ideation, highlighting the need for longitudinal studies to assess how these factors evolve over time. Third, while the study controlled for age, sex, and depression, other potential confounding variables—such as substance use, PTSD, work shifts, and medication use—were not fully explored. Additionally, reliance on self-reported measures (PSQI) may have introduced recall and social desirability bias, potentially leading to underreporting of sleep disturbances and suicidal thoughts. The lack of objective sleep assessments, such as polysomnography or actigraphy, limits the ability to examine physiological sleep disruptions. Furthermore, findings may not be generalizable to other military branches, as sleep conditions and risk factors may differ. Lastly, the stigma associated with suicide in military environments may have encouraged the underreporting of suicidal ideation, affecting the accuracy of prevalence estimates.
In conclusion, this study highlights a significant association between sleep disturbances and suicidal ideation among Mexican naval personnel. These findings suggest that sleep problems may play a direct role in suicide risk rather than merely reflecting depressive symptomatology. Future research should include larger, more diverse samples, utilize longitudinal designs, incorporate objective sleep measures, and address additional psychological and environmental factors to improve the understanding of sleep-related suicide risk in military populations. Prospective studies measuring baseline sleep quality of military personnel from the moment of recruitment are required to be able to estimate risks with greater validity and accuracy as they progress through military life. Efforts should be made to reduce the stigma surrounding suicide in military populations to improve the accuracy of self-reported data. Finally, developing and implementing targeted interventions addressing both sleep disturbances and mental health issues could significantly enhance suicide prevention strategies in military settings.