INTRODUCTION
Eating Disorders (ED) are serious psychiatric illnesses (American Psychiatric Association [APA], 2013; Klump et al., 2009) associated with concern with body weight or shape, and subsequent behaviors designed to achieve weight loss such as dietary restriction, binge eating, compensatory behavior such as food restriction, laxative use, induced vomit, and overtraining (Culbert et al., 2015). Disordered Eating Behaviors (DEB) are inappropriate behaviors characteristic of ED that do not meet the necessary diagnostic criteria (Unikel-Santoncini et al., 2010).
EDs predominantly affect women aged 13 to 25, the diagnostic ratio being10 females for every male (Erriu et al., 2020). According to data from the National Psychiatric Epidemiology Survey (Medina-Mora et al., 2003) conducted in the adult population, bulimia nervosa (BN) affects 1.2% (.6% of males, 1.8% of females) of the adult population.
Regarding the undergraduate population, studies from various countries have reported wide-ranging results regarding the prevalence of DEBs. For example, a study of Chilean students found that 16.9% of women and 8.7% of males are at a high risk of developing DEBs, while 25.6% of women and 33.8% of men are at a moderate risk (Escandón-Nagel et al., 2021). A study conducted in Spain reported that 19% of the population are at risk of developing EDs, including 21.2% of women and 15% of men. In Greece and Colombia, risk levels are between 44.1% and 61.1% for females, and between 9.6% and 38.9% for males (Martínez-González et al., 2014). Among Peruvian medical students, the risk of developing DEBs was found to be 12.5%, 31.7% for women and 10.8% for men (Zila-Velazque et al., 2022). (Mendoza & Olalde, 2019). A study of a representative sample of medical students in Mexico (Mendoza & Olalde, 2019) found that 8.6% were at high risk of DEBs, and 23.5% were classified as being at moderate risk. This was measured using the Brief Questionnaire for Measuring Disordered Eating Behaviors (Unikel-Santoncini et al., 2004). More males tended to be classified as high-risk (9.4% vs. 7.4%), whereas more females were classified as moderate risk (28.4% vs. 19.8%). The study also found that 5.9% of participants used diet pills, 1.6% used diuretics and .5% used laxatives (Mendoza & Olalde, 2019). A study conducted in Mexico City observed a DEB prevalence of 6.8% in females and 4.1% in males (Díaz de León-Vázquez et al., 2017). Conversely, a comparison of DEBs between Mexican and Canadian women found that the percentage of women at risk for developing DEBs was 17.7% and 4.5% respectively (Saucedo et al., 2017).
The etiology of EDs is complex and heterogeneous, involving both genetic and environmental factors (Mitchison & Hay, 2014). The interaction between temperament, early life relationships and life experiences may determine whether a person develops an ED (Le et al., 2017). In regard to environmental factors, sociocultural models highlight the beauty standards or ideals of extreme thinness and objectification for women in western culture as specific risk factors for ED (Striegel-Moore, et al., 2007).
The Tripartite Influence Model posits that sociocultural pressure regarding appearance can be divided into three sources: peers, family, and the media. The model proposes that this pressure is a crucial factor in the development of body image and eating disorders, through the internalization of the thin body ideal. This is compounded by the subsequent comparison of one’s own physical appearance with this ideal (Keery et al., 2004; Schaefer et al., 2019).
Family characteristics constituting risk factors for ED development have been detected. Families of patients with EDs have been identified as more dysfunctional than those without ED. Patients with EDs describe their families as having low cohesion, and poor adaptability and communication, compared to those of participants without EDs (Sainos-López et al., 2015). Furthermore, overprotective behaviors have been observed in parents of anorexia nervosa patients (Le Grange, 2009). Family criticism of weight and body shape, low cohesion, and high parental expectations have been recognized as antecedent factors of bulimia nervosa development, compared to control groups with mixed psychiatric disorders or no psychiatric disorders (Le Grange, 2009).
Family pressure to be thin has mainly been measured through isolated questions within larger questionnaires. Few questionnaires exist that specifically measure sociocultural pressure to be thin. For example, the Influence of Body Aesthetic Models Questionnaire (Spanish acronym CIMEC), validated in Mexico (Vázquez et al., 2000), measures the influence of situations and agents promoting the current aesthetic model. This questionnaire, however, has only one question about family pressure to be thin: “Do you talk to family members about weight-losing activities or products?”. Conversely, the Sociocultural Attitudes Towards Appearance Questionnaire (SATAQ-4) includes a four-question subscale measuring family pressure to be thin. The third version of this questionnaire was validated in male Mexican undergraduates (Castillo et al., 2019). However, this version does not include questions specifically exploring comments by different family members, and the validation study did not include females.
Given the lack of a culture-specific psychometric instrument for measuring family pressure to be thin in a sample of Mexican undergraduates, a questionnaire was expressly designed for this purpose. Construct and convergent validity with SATAQ-4 was obtained together with a comparison with a clinical sample. Total reliability and test-retest reliability with a three-week period between responses were also calculated. Sex comparisons were made with all the variables included in the study. Both the clinical group and non-clinical were expected to obtain high scores in all variables.
METHOD
Participants
The eligibility criteria for the sample were being Mexican university students, being over 18, and being enrolled at a public or private Mexican university. Participants were selected through non-probabilistic convenience sampling.
The sample comprised 478 students, female (n = 259), male (n = 104), non-binary (n = 2), and unspecified (n = 4). Participants were enrolled in universities in Mexico City; Mexicali, Baja California; Villahermosa, Tabasco; Zacatecas, Zacatecas; and Morelia, Michoacán. Thirteen subjects did not agree to sign the informed consent form, 39 failed to meet the inclusion criteria and 57 answered the attention checks incorrectly, leaving a total of 369 participants (70.2% women, 28.2% men, .5% non-binary, 1.1% preferred not to answer). The average age was 20.75 (SD = 2.72), with an age range of 18 to 45, with no statistical differences between genders (women/men/nonbinary/did not answer). Ninety-three point two percent of participants were single, 4.3% were in a common law union, 2.2% were married and .3% were widowed. The sample comprised students from 19 universities in Mexico (n = 10 public schools and n = 9 private schools).
To obtain test-retest reliability, questionnaires were administered to the same individuals three weeks after the first time, with responses being obtained from 60 participants (68.3% women/28.3% men/1.7% non-binary/1.7% preferred not to answer).
The clinical sample comprised 50 subjects (39 women and 11 men), 11 of which were patients undergoing treatment for an eating disorder. Thirty-nine were undergraduate students who answered the question “Have you been diagnosed with an eating disorder?” affirmatively and specified that they had a diagnosis defined by the Diagnostic and Statistical Manual of Mental Illnesses (DSM-5) (APA, 2013). Those who said that they had DEBs, ate due to depression, or bigorexia, were excluded. The average age for the clinical sample was 21.54 years (SD = 2.70), with an age range of 18 to 43, 96% were single and 4% were in a common-law union. No statistically significant age differences were found between the student group and the clinical group.
Instruments
The Brief Questionnaire for Measurin Disordered Eating Behaviors (BQDEB) comprises 10 items exploring concern about gaining weight. It also examines the feeling of lack of control when eating, and restrictive, purgative and binge eating behaviors, in the past three months and was validated in Mexican clinical and student populations (Unikel-Santoncini et. al., 2004). A recent factor analysis obtained a Cronbach’s alpha value of .76, and 64.7% of explained variance, divided into the following three factors: binge eating/purging, compensatory measures, restriction (Padrós-Blázquez et al., 2022).
The Social Attitudes towards Appearance Questionnaire (SATAQ-4) (Schaefer et al., 2015) was validated in the Peruvian (Zevallos-Delzo et al., 2017) and Colombian population (Villegas et. al. 2021) but has not yet been validated in Mexico. The instrument is divided into two factors. Internalization is the degree of acceptance of physical appearance expectations and stereotypes and includes the areas of thinness/low adipose index, muscularity, and general attractiveness. Pressure measures the level of perceived interference from various groups regarding their physical appearance. It includes family, peers, significant others, and the media (Schaefer et al., 2015). This questionnaire has four items specifically related to family pressure: “I feel pressure from my family members to look thinner,” “I feel pressure from my family members to improve my appearance,” “My family members encourage me to reduce my body fat level,” and “My family members encourage me to get in better shape.” Because this scale contains specific items about family pressure in the context of EDs, it is relevant for the validation of this scale. In the sample in this study, it obtained a reliability of .81 and was organized into a single factor explaining 64.11% of total variance.
The Family Pressure To Be Thin Questionnaire consists of 42 questions in Likert format, with five response options: 1-Never, 2-Almost never, 3-Sometimes, 4-Frequently and 5-Always. A higher score indicates greater pressure from the family regarding weight and body shape. Two attention checks were added to detect random responses, in the following format “If you are answering this questionnaire correctly, select the option “Frequently”.
Procedure
The study was divided into three parts: Phase 1) Selection and inclusion of items; Phase 2) Construct validity; and Phase 3) Concurrent validity.
Phase 1
A bibliographic study was conducted of sociocultural pressure from the family on weight and body shape and the development of disordered eating behaviors. Fourteen questions were devised to conduct a semi-structured interview for university students (such as Does anyone in your family diet? How much importance do they give to weight and body shape in your family?). With these questions, eight interviews were conducted and subsequently analyzed to develop the 42 questions in the instrument.
Three experts on EDs were asked to evaluate the pertinence, relevance and conceptual clarity of each of the items comprising the instrument. They recommended including all the questions with certain modifications, such as adding “obesity” in all the sections including the term “overweight”. With the resulting version, a cognitive laboratory (n = 16, 13 women and three men) was organized with undergraduate students to check their understanding of the content and structure of the questionnaire.
A pilot study was subsequently conducted (n = 27) with undergraduate Mexican students, the response time was recorded, and a Cronbach’s alpha reliability of .95 was calculated. This yielded a final version of the questionnaire which was subsequently tested with a sample of undergraduate students at Mexican universities to obtain its reliability and validity.
Phase 2
Responses were collected through a digital survey on the Office Forms platform between February and March of 2024; the questionnaire was shared with professors from various universities in Mexico so that they in turn could share it with their students. Analyses were conducted to obtain exploratory and confirmatory factorial validity; the latter considered both first and second order analysis.
Phase 3
The concurrent validity of the instrument designed with the Family Pressure Subscale of the SATAQ-4 and the BQDEB was obtained. Likewise, comparisons were made for each of the variables studied, by clinical group vs. student group, and by sex.
Statistical analysis
Frequencies and percentages of demographic variables (gender, career, parents’ educational attainment, public or private school) were obtained, as well as the mean and standard deviation of the age variable. The sample was randomly divided into two groups. One comprised 60% of participants (n = 219) to conduct the exploratory factor analysis (Field, 2009), and the other comprised 40% (n = 150) to conduct the confirmatory factor analysis (Brown, 2015). The first sample met the quota of five to 20 participants for each survey item (Campo-Arias & Oviedo, 2008; Sánchez & Echevarry, 2004) while the second complied with the minimum of 150 subjects for confirmatory factor analysis (Wang & Wang, 2012). Item-total correlations were obtained considering a correlation of .20 or greater to retain an item according to the criterion proposed by Streiner and Norman (2008). In the exploratory factor analysis, we followed Yela’s criteria (1997): 1) An item must have a saturation equal to or greater than .40; 2) An item is only included in one factor, the one in which it has a higher level of saturation; 3) There must be conceptual congruence between all the items included in a factor; 4) A factor must comprise at least three items. The reliability of the instrument and its factors was obtained with Cronbach’s alpha and the three-week test-retest reliability was obtained with a bivariate correlation analysis.
The DWLS estimation method was used to conduct the confirmatory factor analysis of both the first and second order . The goodness-of-fit criteria for the first-order CFA were RMSEA ≤ .08, CFI ≥ .95, TLI ≥ .90, GFI ≥ .90 and SRMR ≤ .08 and probabilities, Z values and variance estimates were reported for the second-order CFA.
Since the family pressure subscale of the SATAQ-4 questionnaire has not been validated in Mexico, Cronbach’s alpha reliability and the factorial structure of principal components with Varimax rotation were obtained. Bivariate correlations were performed with the total sample of students between DEBs, the Family Pressure To Be Thin Questionnaire, and the family pressure subscale of the SATAQ-4. Finally, we compared the sum of each instrument for the total sample of students with the sample with EDs, using a Student’s t for independent samples, and a one-way ANOVA for the comparison by sex (eliminating subjects who preferred not to answer). Analyses were conducted in SPSS for Windows version 21 (IBM, 2012) and JASP (JASP team, 2020).
Ethical considerations
The project was approved by the Ethics Consulting service of the Anahuac University in Mexico. An informed consent form was designed for all the activities where information was collected and sent to all participants digitally prior to all activities.
RESULTS
Phase 2 Exploratory factor analysis
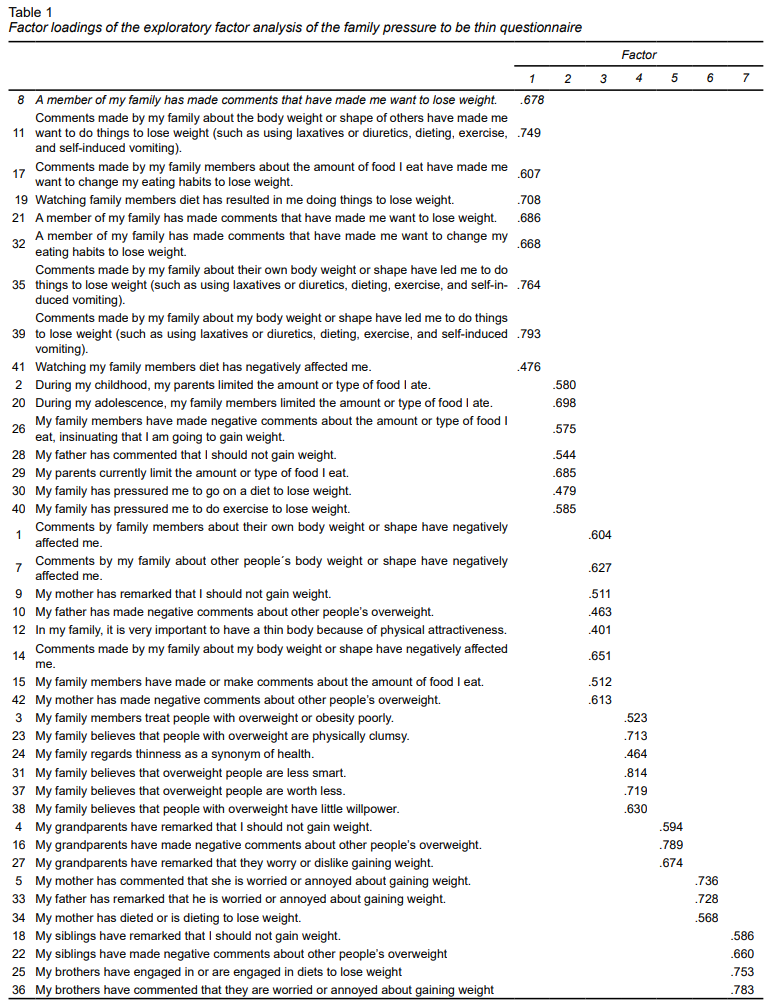
Item-total correlations were obtained, and since all the items showed values greater than .20, they were all included for exploratory factor analysis. A principal components analysis with Varimax rotation was conducted, yielding an eight-factor structure explaining 66.67% of variance (see Table 1). Factor 1, comprising 10 questions, was called “Negative comments directed at the individual’s physique.” Factor 2, consisting of nine questions, was called “Pressure to change an individual’s eating behavior.” Factor 3, including eight questions, was called “thin ideal-reinforcing comments.” Factor 4, containing six questions, was called “Family beliefs about being overweight”; Factor 5 and 6, each comprising three questions, were called “Pressure from grandparents” and “Parental concern about being overweight” respectively. Factor 7, comprising four questions, was called “Sibling Influence.” Factor 8 included two questions, including number 24, which also loaded on factor 4, with which it had conceptual coherence. Question 13 was eliminated from the questionnaire as it failed to meet the necessary requirements to form a factor (Yela, 1997). Question 6 was excluded from the analysis.
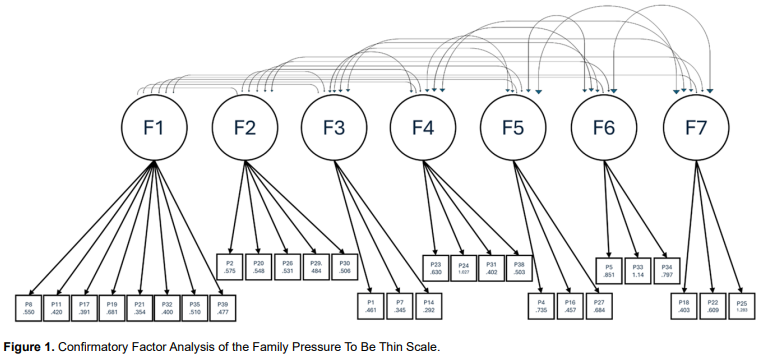
Confirmatory factor analysis
The first order confirmatory factor analysis yielded a seven-factor structure (see Figure 1) showing adequate goodness of fit: RMSEA =1.00, 90% CI [= .00]; CFI = 1.00; TLI = 1.03; GFI = .98; SRMR = .056; Chi² (χ2 =140.89, df = 356, p = 1.00). All items obtained statistically significant loads within their factors, with Z values between 7.06 and 30.73, all of which were statistically significant (p < .001). There were no modified or residual covariance indices once items 2, 3, 9, 10, 12, 15, 28, 36, 37, 41 and 42 had been eliminated. The final distribution of the items by factor was as follows: 1) questions 8, 11, 17, 19, 21, 32, 35, and 39; 2) questions 2, 20, 26, 29, and 30; 3) questions 1, 7, and 14; 4) questions 23 , 24, 31, and 38; 5) questions 4, 16, and 27; 6) questions 5, 33, and 34; 7) questions 18, 22, and 25 (see Appendix1. for the final version of the questionnaire in Spanish.
Second-order confirmatory factor analysis
Second-order confirmatory factor analysis yielded a unidimensional solution, leaving seven factors as in the first-order solution. All factors showed a probability of less than .001, with Z values ranging from 5.05 to 9.76, and variance estimates ranging from .66 to 1.82.
Reliability
The reliability of the scale and its factors was obtained, as well as the three-week test-retest reliability. The scale obtained a Cronbach’s Alpha value of .94, .94 for factor 1, .85 for factor 2, .90 for factor 3, .79 for factor 4, .77 for factor 5, .66 for factor 6 and .63 for factor 7. The three-week test-retest reliability coefficient for the total scale was .86. In the second-order confirmatory factor analysis, a Cronbach’s alpha value of .94 was obtained with a confidence interval of between .93 and .95.
Phase 3 Convergent validity
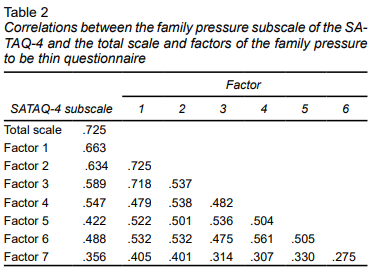
Convergent validity was obtained by correlating the family pressure subscale of the SATAQ-4 with the total scale and factors of the Family Pressure To Be Thin Questionnaire. The results showed that all of them were statistically significant (p < .01) and greater than .40 except for factor 7 of the scale and the SATAQ-4 Family Pressure Subscale (see Table 2).
Comparison between Clinical and non-clinical groups
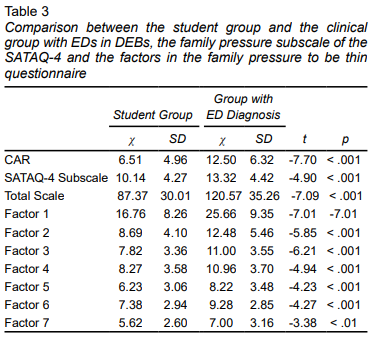
The student group and the clinical group were compared in regard to DEBs, the family pressure subscale of the SATAQ-4 questionnaire and the factors in the Family Pressure To Be Thin Questionnaire. The results showed statistically significant differences in all the variables measured with higher scores in the clinical group than in the student group (see Table 3).
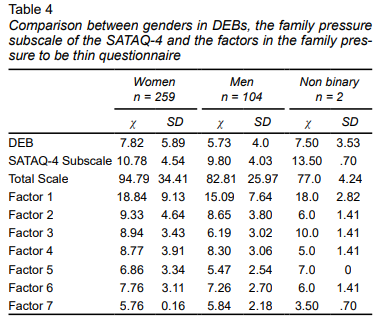
Comparisons by gender
The gender comparison showed that the non-binary group scored almost as high as women in the DEB variable, factor 1, and higher in the Family Pressure Subscale of the SATAQ-4. This group also scored higher in factors 3 and 5 of the Family Pressure To Be Thin Scale, followed by the group of women, with the exception of factor 7, in which men scored higher. Statistically significant differences were found in DEBs, the total Family Pressure To Be Thin Scale and factors 1, 3 and 5 of the same scale (see Table 4).
DISCUSSION AND CONCLUSION
The process of elaboration and validation yielded a 29-item instrument divided into seven factors. Answers to these items correlated with the Family Pressure To Be Thin Subscale in the SATAQ-4. The data fit the model and good total and test-retest reliability was obtained, showing that the instrument has adequate psychometric properties for the sample studied. The results showed that the structure and content of the items fit the family component of the tripartite theoretical model (Keery, 2004), covering the behaviors mentioned in this theory such as criticism of weight and body shape and eating habits. The Family Pressure To Be Thin Questionnaire is a reliable, valid instrument which can be useful for assessing the risk of developing eating disorders.
The clinical group scored higher on all the variables studied than the control group, which is consistent with other studies recognizing family pressure as a risk factor in the development of DEBs and EDs (Mitchison & Hay, 2014). This is consistent with the high parental expectations and higher incidence of family criticism of weight and body shape observed in families of patients with BN (Le Grange et al., 2009). It suggests that family pressure constitutes a risk factor for the development of eating disorders. Likewise, these results point to the relevance of contextualizing an individual’s family environment when investigating an ED, and as a factor in treatment and prevention. Interventions designed to improve family dynamics and reduce criticism of an individual’s body image and diet can be crucial in a comprehensive approach to eating disorders (Fuentes Prieto et al., 2020).
In a sample of American, Australian, Italian, and British university women (aged 17 to 30), the Family Pressure on Appearance Subscale of the SATAQ-4 was found to correlate significantly with the measurement of DEBs, body dissatisfaction and self-esteem. Similarly, in the present study, higher scores were found in the clinical group than the non-clinical group across all measurements (Schaefer et al., 2015).
The SATAQ-4 has also been adapted for men considering masculine beauty ideals (Schaefer et al., 2015). The questionnaire in the present study showed adequate reliability and validity values in women and men. However, the sample of men was not large enough to conduct a separate analysis by sex, which does not allow us to replicate the findings of this widely used instrument.
A study measuring family pressure on appearance in healthy women with an average age of 21 years found that neuroticism is related to critical comments towards children and the expression of certain values in that respect. It concludes that a negative effect only occurs when children display some form of vulnerability, as borne out by theories on multifactorial influences in the etiology of EDs (Davis et al., 2004).
A systematic review of family pressure contributing to the development of eating disorders in the Asian population (Sun et al., 2023) found that pressure exerted by the mother is the variable with the greatest influence on the development of EDs. In general, it has been reported that parental criticism has a direct influence on the practice of dieting and weight loss in university students as found in the present study. Nevertheless, our study does not include specific questions on the pressure exerted by mothers (Chng & Fassnacht, 2016; Rodgers et al., 2009; Wertheim et al., 2002).
The study conducted by Ordaz et al. (2018) found that in women of Hispanic origin in the United States, pressure from family and the media is a key factor in the development and maintenance of eating disorders. This was also observed in another study on the central role played by the family in Hispanic culture in the development and maintenance of eating disorders (van den Berg et al., 2008). The tripartite model posits the influence of the media, family and peers in the development of DEBs and EDs. In Mexico, a country with high percentages of overweight and obesity (Barquera et al., 2024), where the family occupies a central role, it is important to measure the pressure the latter exerts on the development of DEBs and EDs.
The fact that women scored higher than men on factors 1, 2, 3, 4, 5, and 6 suggests that women experience greater family pressure to be thin than men. This is congruent with the higher incidence of both ED and DEB in women, consistently identified in national and international literature (Erriu et al., 2020; Medina-Mora et al., 2003; Escandón-Nagel et al., 2021; Martínez-González et al., 2014; Zila-Velazque et al., 2022; Mendoza & Olalde, 2019; Unikel-Santoncini et al., 2004; Díaz de León-Vázquez et al., 2017). It also provides a possible explanation for the difference in the incidence of EDs between genders. It highlights the fact that the ideal of beauty in women is prevalent in today’s society, fostering the desire for thinness, whereas in men it is less prevalent given that the male body ideal tends towards increased muscle mass (Marcos Quiles et al., 2013).
People who self-identified as non-binary scored higher on nearly all the variables measured than women. These results suggest that non-binary individuals experience more family pressure to be thin than men and women. These results are congruent with the rate of 4.7% of non-binary people with a professional diagnosis of EDs (Diemer et. al., 2018). This is higher than the rates for men and similar to that of women, meaning that as a group, non-binary people are at a higher risk of developing ED, at least in comparison with men. However, since there were only two non-binary individuals in this study, further research with a representative non-binary sample is required to confirm this finding.
Regarding the different types of validity assessed with the questionnaire in our study, it is important to note that the modifications proposed by the experts consulted mainly involved adding obesity in addition to overweight. They also involved ensuring that the language did not include words that could be interpreted as offensive or aggressive. In general, the authors regarded the questions as pertinent, relevant and clear, and considered that they adequately covered the construct they were designed to measure.
In regard to construct validity, the instrument measures the variable it is intended to measure since the explained variance exceeded 50% (obtained value = 66.67%). In other words, this is not due to chance and each item is selected to develop the operational definition, so that the instrument has construct validity. Conversely, the results of the concurrent validity of the instrument show that the same construct is being measured with an external parameter, the family pressure subscale of the SATAQ-4, an instrument widely used in international research. This shows that the instrument adheres to what was previously theoretically established. Likewise, the fact that higher values were obtained in the clinical sample than in the non-clinical sample, and with statistically significant differences, indicates that there is an association between the constructs and the pathology studied. The results of the second-order confirmatory analysis indicate that the instrument has adequate psychometric characteristics, making it a useful tool in the study of family pressure to be thin in Mexican university students.
This instrument allows us to measure a factor in the development of eating disorders that was previously impossible to measure in depth. At least in Mexico there are only isolated questions in various questionnaires (Schaefer et al., 2015; Unikel-Santoncini et al., 2004) to measure this construct. The Family Pressure To Be Thin Scale is useful for diagnosing the risk of DEBs and EDs in academic, institutional and health contexts. It measures a construct previously identified as a risk factor for EDs (Le Grange et al., 2009; Keery et al., 2004; Schaefer et al., 2019), which will allow the design of more accurate prevention and intervention programs. It will also allow for more research and understanding of the DEBs and EDs phenomena.
The non-probabilistic convenience sample constitutes the greatest limitation of the present study, since it prevents the generalizability of the use of the scale developed to the entire population of Mexican university students. This study included an exploratory factor analysis of the Family Pressure To Be Thin Subscale of the SATAQ-4 questionnaire to obtain convergent validity. However, it would also be important to validate the questionnaire with a different sample and corroborate its validity. At the same time, the self-report format of this questionnaire poses a risk of response bias due to social desirability or lack of motivation (del Valle & Zamora, 2021). It would be useful to administer the questionnaire to other populations, and to obtain its predictive and divergent validity. Validating this psychometric instrument with a probabilistic and representative sample of the population, and exploring divergent validity and predictive validity could enhance its psychometric qualities and usefulness and relevance for statistical, clinical and research-focused applications. In conclusion, the modified, validated questionnaire obtained adequate psychometric characteristics, making it a brief, useful tool for examining the relationship between family pressure and other constructs associated with mental health in the Mexican university population.