INTRODUCTION
Hearing loss (HL) is characterized by the inability to identify sounds below standard hearing thresholds (Lieu et al., 2020). Approximately 1.57 billion people have HL globally, a figure that is expected to rise to 2.45 billion people by 2050 (Haile et al., 2021). HL prevalence in Colombia is 4.3 per 1000 individuals under 10 (Vargas Dìaz & Neira Torres, 2015). Children and adolescents with HL may have delayed language development, compromising their performance in a variety of everyday tasks, particularly those related to executive function (EF). This is an integrated set of abilities resulting in a coordinated, flexible approach to achieve specific goals (Tirapu Ustárroz et al., 2008).
EF skills development is affected by a range of environmental factors, among which language acquisition may exert the strongest influence (Botting et al., 2017). Cognitive processes such as naming, categorization, generalization of the surrounding environment, and the capacity for abstraction are fostered by language (Svirsky et al., 2000), strengthening verbal and non-verbal task performance related to EF (Castellanos et al., 2016). Deaf children who have experienced a period without full access to both auditory and linguistic input have been found to experience greater difficulty in developing their EF, compared to their cochlear implant using peers (Hall et al., 2018; Figueras et al., 2008).
Surowiecki et al. (2002) underlined the association between attention, performing continuous tasks, and EF. In hearing-impaired children, attentional functions may be impaired or altered due to the differences in information processing. The absence of hearing input overloads the visual system affecting the ability to perform tasks properly. Moreover, Mitchell and Quittner (1996) considered that impairments in continuous performance tasks could be due to impaired cognitive abilities and difficulty determining which stimuli are targets and which are not. Both theories support and attempt to explain the concept of an increased risk of developmental impairment and poor task performance in children with HL compared to their normal-hearing peers (Kirby et al., 2019).
Several studies have shown that, compared with their normal-hearing peers, children and adolescents with both unilateral and bilateral HL experienced greater difficulty in tests of working memory, inhibition, cognitive flexibility, and attention (Figueras et al., 2008; Hall et al., 2018; Kirby et al., 2019; Kronenberger et al., 2013; Surowiecki et al., 2002). However, there is a dearth of studies focused on the Latin American, specifically Colombian pediatric population with HL and their EF performance. Moreover, there are a limited number of publications evaluating EF through neuropsychological tests adapted for the Spanish-speaking population.
The aim of this study is therefore to determine EF performance in a population of children and adolescents with prelingual HL in Bogotá D.C, Colombia. It also seeks to describe the relationship between EF performance and individual HL characteristics such as the length of hearing aid or cochlear implant use, degree, etiology, and type of HL.
METHOD
Study design
A cross-sectional observational study was conducted according to the STROBE guidelines for cross-sectional studies.
Setting
The study was conducted at Fundación CINDA (Centro de Investigación e Información en Deficiencias Auditivas) (Center for Research and Information on Hearing Impairment) in Bogotá, Colombia. This center attends the hearing-impaired population through a multidisciplinary rehabilitation program focused on the development of communication skills. Most children at this center had either a cochlear implant or some sort of hearing aid and had attended therapy from an early age. Individuals at CINDA receive therapy based on the auditory-verbal therapy (AVT) methodology (Brennan-Jones et al., 2014). This type of therapy uses acoustic phonetic stimulation, designed to develop children’s perception and auditory discrimination skills to achieve normal language development.
Participants
Participants were included on the basis of the following criteria: being aged between 5 and 16, prelingual HL (HL diagnosed before language acquisition), attending in-person therapy at the CINDA foundation who were also enrolled in regular schools, and providing written parent consent. Exclusion criteria included not having parental consent to participate in the study, individuals with post lingual HL, chronological age outside the established age range, concomitant diagnosis of intellectual disability as borne out by their medical records, and attending virtual-modality therapy. A total of 70 children were eventually selected for the study. Those who did not meet the inclusion criteria were excluded from the study.
Intellectual disability can impact an individual’s performance in cognitive and executive function tasks. Individuals with hearing loss and concomitant intellectual disability, as according to their medical records, were therefore excluded from the study. To rule out intellectual disability, an initial evaluation was conducted by a multidisciplinary team comprising psychologists, speech-language pathologists and occupational therapists with experience working with children with HL. Standardized tests are used in each discipline to place children in age groups for motor development, communication and intellectual functioning. For the latter, the institution’s psychologists use the WISC-R with the appropriate scores for the HL population.
A previous study showed a mean Complex Figure Retrieval score of 9.40 with a standard deviation of 3.91 (Rosselli-Cock et al., 2004). Taking an absolute accuracy of 10% to estimate this mean with an alpha of .05 yielded a sample size of 66 participants. Seventy participants were eligible and completed the tasks.
Measurements
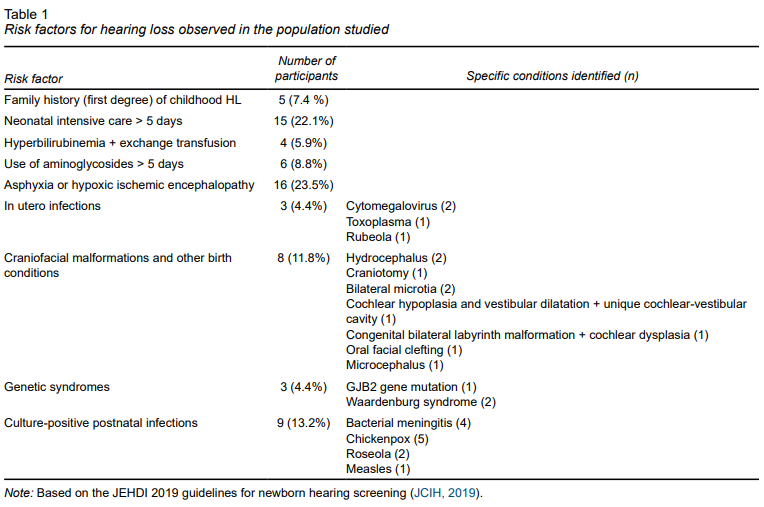
Clinical and demographic factors were extracted from medical records at Fundación CINDA. Regarding HL, the following aspects were recorded for each participant: age at diagnosis, determined by the date of the hearing test or evoked potential reports; degree of HL, according to criteria defined by the American Speech-Language-Hearing Association (ASHA) (Clark, 1981); type of HL (conductive or neurosensorial) and laterality of HL (unilateral or bilateral) determined at the time of diagnosis and outlined in the medical records; type and model of hearing aid, and length of device use determined by the date of surgery in the case of cochlear implants or by the date of first programming for hearing aids. Risk factors for congenital HL were determined in accordance with the Joint Committee of Infant Hearing criteria (JCIH, 2019).
Each participant entered the examination room accompanied by one of their parents, where they was asked by a trained examiner to perform a series of selected EF tasks for approximately one hour. Examiners included a medical doctor with previous research experience in studies with children with neurodevelopmental and hearing disorders and three medical students, all of whom were trained to conduct the tests by an experienced psychologist in the field. Afterwards, parents were able to clarify issues regarding their children’s performance. Finally, results were collected in an Excel database for subsequent statistical analysis.
The Child Neuropsychological Evaluation 2nd Edition, known in Spanish as ENI-2, evaluates neuropsychological development in children and adolescents between 5 and 16. It is the first of its kind adapted to the Latin American pediatric population. The ENI-2 measures performance in thirteen cognitive areas including attention, constructive skills, memory (encoding and delayed recall), perception, oral language, metalinguistic skills, reading, writing, visuospatial skills, conceptual skills, and EF (Matute et al., 2014). The ENI-2 demonstrated good reliability through procedures such as test-retest, inter-rater reliability, and correlations with other psychometric tests such as the Wechsler Intelligence Scale for Children (WISC). It has also proven useful in the evaluation of various populations, including children with attention deficit hyperactivity disorder and learning disorders. Considering the particular characteristics of the population studied, only six cognitive subtests were chosen out of the thirteen available tests. We selected three domains that directly evaluate EF including fluency (verbal and graphic), cognitive flexibility, and planning and organizing, in addition to visual memory and visual attention subtests. We did not include subtests with a higher verbal component such as the verbal fluency and verbal memory subtests given that the population consisted of children and adolescents with HL. In addition, we did not include a large number of studies to prevent fatigue and distractibility in participants (Matute et al., 2013). These included the following:
Constructive skills: The examiner presented a complex geometric figure to participants who were asked to copy it as accurately as they could. The drawing was scored according to the number of correct elements included. The maximum score was 12 points for children between 5 and 8 and up to 15 points for children aged 9 to 16.
Visual memory (encoding): Participants were shown a series of geometric figures one by one. Each figure was shown for approximately one second. After all the figures had been presented, the participant was asked to draw the figures they remembered. This was repeated three more times. The number of correct figures was registered, the maximum score in each trial being 12 points for children aged 9 to 16, and 9 for those aged5 to 8. Examiners also evaluated the presence of intrusions, the inclusion of figures outside the original series, as well as perseverance, the repetition of a figure already included in the same trial.
Visual memory (recall): 30 minutes after copying the complex figure, participants were asked to recall and draw the mentioned figure as accurately as they could.
Visual attention: Participants were presented with a standardized matrix containing large and small animal silhouettes. They were asked to cross out the larger animal figures in the matrix. A point was awarded for every large animal crossed out, and a point was deducted for every small animal crossed out, with a perfect score of 44 points for all age groups.
Planning and organizing: Participants were presented with three differently colored and sized wooden blocks. They were shown different configurations in which the blocks could be assembled and asked to replicate them with the fewest number of movements. A point was awarded for every correct construction made with the fewest number of movements, for a total of 11 points for all age groups.
Non-semantic graphic fluency: Using a standardized matrix, participants were asked to draw as many different designs composed of four lines only. A point was assigned for every correct design making a total of 34 points for all age groups.
Cognitive flexibility: Using the feedback (correct or incorrect) provided by the evaluator, participants were asked to identify the principle (color, shape or number) underlying the grouping of a set of 54 cards. The number and percentage of correct answers was registered.
A raw score was obtained after each subtest had been conducted. Raw scores were converted to their equivalent normative scores (T score, percentile, scalar score) using the normative tables provided by the ENI-2 application manual. Although ENI-2 score systems are different for each age group (5 to 8 and 9 to 16 years old), the raw score obtained by each participant was subsequently converted to its equivalent normative score (T score, percentile, scalar score) allowing its comparison with an age-matched normative sample. Comparisons were made directly with established normative scores, rather than with each other. As indicated in the application manual, percentiles were then categorized as follows: percentile > 84 (Superior), 84 (High average), 26-75 (Normal or average), 16 (Low average), 5-9 (Limit), ≤ 2 (Very low) with higher percentiles indicating better performance. Percentiles were used in statistical analysis as both a continuous and a categorical variable.
Statistical analysis
Data were recorded in a Microsoft Excel format. Raw scores obtained by each participant for each EF domain (visual attention, visual memory-encoding, visual memory-recall, cognitive flexibility, constructive skills, non-semantic graphic fluency, planning and organizing) were converted to standard scores (scalar score, T score and percentile) according to the normative score tables by age provided by the ENI-2 Application Manual (Matute et al., 2013). Statistical analysis was performed using STATA v18.5. Data were tested for normal distribution with the Shapiro-Wilk normality test. We used arithmetic mean and standard deviations for quantitative variables, and percentages and simple frequency distribution to describe qualitative variables. Given that the outcome variables did not follow a normal distribution, we performed non-parametric tests for variable comparison (Mann-Whitney test for 2-category variables and Kruskal-Wallis test for > 2 category variables). A p < .05 was considered significant.
A subgroup analysis was performed, categorizing each outcome variable (EF percentile) into group 0 (percentile 15 or less) and 1 (percentile > 15). This allowed direct comparison between individuals who had achieved an average or above average median score with those who had achieved a lower-than-average score. Additionally, we tested subgroups by degree of HL (moderate, severe, profound) to evaluate potential changes in the median subtest scores with increasing HL severity.
Ethical considerations
This is a study with minimal risk in accordance with resolution 008430 issued in 1993 (“Scientific, technical and administrative standards for health research”) by the Colombian Ministry of Health. It follows national legal and ethical guidelines as well as those contemplated in the latest modification (World Medical Association [WMA], 2013) of the Declaration of Helsinki of the WMA (“Ethical principles for research involving human subjects”). This study was approved by the ethics committee at Universidad del Rosario with approval number DVO005 1825-CV1512.
RESULTS
A total of 70 participants were evaluated, including 34 girls (48.6%) and 36 boys (51.4%) aged between 5 and 16 with a mean age of 10.25 ± 3.02 years (range 5.2 to 15.8). According to the type of HL, only two participants (2.9%) were diagnosed with conductive HL, 67 with neurosensorial HL (95.7%), and one remained unclassified due to the lack of information in their medical records. Most participants had profound (80%), followed by severe (10%) and moderate HL (4.3%). No information in medical records regarding the degree of HL was available for four individuals (5.7%). Almost all participants had bilateral HL (97%), except for two who had unilateral HL (3%). Regarding the type of hearing aids, 53 of the 70 participants were cochlear implant users (75.7%), 18 out of 70 used hearing aids (25.7%), 17 used both (24.3%), and only three used a bone conduction system (4.3%). Age at diagnosis, as determined by a complete audiological evaluation or confirmed by auditory evoked potentials, ranged from one month to four years old. Risk factors for childhood HL in the population evaluated are outlined in Table 1.
HL and EF Performance
A total sample of 70 participants performed each EF subtest. Five participants were unable to complete the subtests for the cognitive flexibility domain, meaning that these data were excluded from the corresponding analysis. Raw scores for all subtests were converted to percentiles according to the age-matched normative samples included in the ENI-2 application manual. Standardized percentiles for each subtest are given in Table 2.
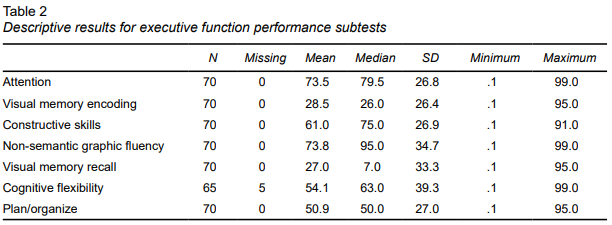
Overall, percentile mean scores for the total population were average or above average for all subtests (Figure 1). Participants scored lowest in the visual memory domains, including both encoding and recall skills, with the highest mean scores being reported for the attention and non-semantic graphic fluency subtests.
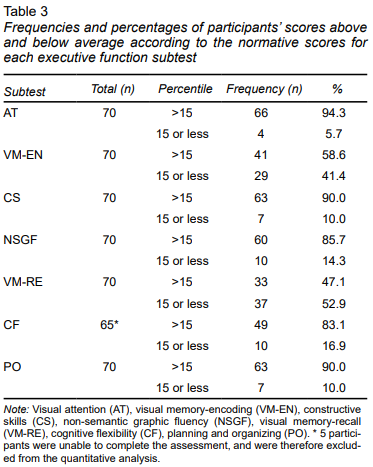
Among individuals who scored below average, 52.9% of participants scored below the 15th percentile for the visual-memory recall subtest, 5.7% for attention, 41.4% for visual memory–encoding, 10% for constructive skills, 14.3% for non-semantic graphic fluency, 16.9% for cognitive flexibility, and 10% for planning and organizing scores (Table 3).
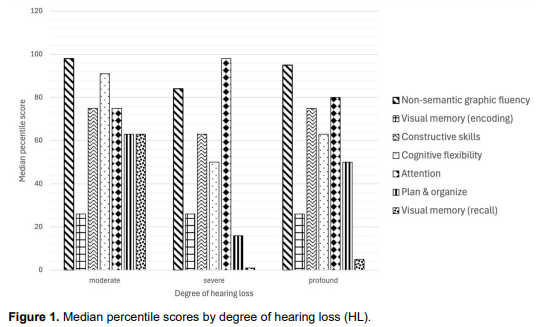
Given that data for EF subtests did not follow a normal distribution, a non-parametric Mann Whitney test and Kruskal Wallis test were conducted to determine the association between EF scores and independent variables (age at diagnosis, chronological age, degree of HL, type of hearing aid and sex). However, no significant differences were found between the variables mentioned and EF subtest performance. Subgroup analysis by degree of HL showed no significant differences in terms of EF subtest performance.
DISCUSSION AND CONCLUSION
This study demonstrated the characteristics of EF performance in children and adolescents with prelingual HL, comprising both cochlear implant and hearing aid users, who were receiving auditory-verbal therapy. Notably, over half the participants obtained normal and even above normal normative scores in most of the domains evaluated, except for the recall memory subtest. Given that subtests were selected due to their limited auditory input, these results could reveal a strength in this population, associated with visual information processing. Nonetheless, participants obtained lower scalar scores in the visual memory tasks, which could be explained by a shorter attention span, distractibility and fatigue due to the duration and complexity of the tasks. These deficits may therefore be attributable to environmental factors, rather than a visual deficit in itself.
Our findings are supported by recent studies comparing 32 children with cochlear implant with their regular hearing peers, using multiple cognitive subtests (De Giacomo et al., 2021). These included forward and backward digit span tests for evaluating working memory, phonemic and categorical fluency subtests for cognitive flexibility, the inhibition and control of the impulse response-Continuous Auditory Feedback (CAF), and The Tower of London Test for planning and organizing. This study demonstrated that children with cochlear implants have significantly lower scores than normal hearing children in all EF domains, which the authors argue may be attributable to the absence of auditory stimuli and hearing deprivation during the perinatal period.
Findings showed no significant correlation between the length of time from diagnosis to device implementation and EF performance. Conversely, one study demonstrated that children with cochlear implant activation at a younger age performed better in working memory and cognitive flexibility domains, which could potentially be explained by the early recovery of auditory input (De Giacomo et al., 2021). Furthermore, this study concluded that hearing correction should be implemented before the age of three and a half in accordance with a critical period of brain plasticity, which enhances auditory capacity and EF development. Moreover, it has been demonstrated that young children with early cochlear implant activation, under two years of age, can develop age-appropriate basic phonological and cognitive skills compared with their normal hearing peers, particularly in regard to the working memory domain (Zhang et al., 2022). This demonstrates that early hearing aid implementation is essential for adequate auditory stimulation and therefore improved performance in EF-dependent tasks.
Apart from hearing deprivation and auditory rehabilitation, language development constitutes an influential factor in the development of EF in children with HL. A recent study found that deficient language tended to increase the percentage of Flanker Interference Effect errors, meaning a decrease in inhibitory control, in 40 children with and without cochlear implants, compared with their normal hearing peers (Merchán et al., 2022). Linguistic development and its impact on EF is therefore determined by multiple factors rather than solely cochlear implant use. These factors include age at cochlear activation, social and environmental factors, appropriate exposure to language during the early years of life, school attendance, constant social interaction, and learning sign language, which contributes to stronger spoken language outcomes after cochlear implant activation (Merchán et al., 2022).
Most of the population evaluated belong to a low socioeconomic status, which limits their learning environment. However, at Fundación CINDA participants have had the opportunity to access integral therapies, including AVT, which focuses on attending, early vocalizing, recognition, feedback, sound locating, memory, sound distance and levels, producing vowels and consonants, speech discrimination and comprehension, short- and long-term memory and memory span (Ashori, 2022). Consequently, individualized integral therapy combined with coordinated communication with families and schools, can guarantee early intervention and facilitate language development and performance in EF.
Moreover, recent reports have considered AVT to be extremely useful for improving EF in children with cochlear implants (Ashori, 2022). This randomized case control study evaluated a group of 36 preschoolers, who received 20 sessions of AVT, with pre- and post-intervention assessments using the Behavior Rating Inventory of Executive Function Preschool Version (BRIEF-P). Findings suggest that AVT enhanced EF in participants in all subscales, including auditory skill, short-term memory, working memory, linguistic processing, planning and organizing.
In addition, a relationship has been proposed between the auditory correction method and EF, as well as speech perception and vocabulary. There is evidence that speech perception in adverse listening contexts is a key variable for linguistic, cognitive, and socioemotional development (Boerrigter et al., 2023). The aforementioned study compared speech perception, language development, and EF in children with severe HL with hearing aids and cochlear implants, finding poorer perception of soft speech in hearing aid users, related to receptive vocabulary and planning difficulties. This provides insights for future research related to EF performance in children with HL who communicate with and without sign language.
The cross-sectional nature and lack of statistical significance of the results make it difficult to determine the exact association between EF performance and HL characteristics (such as degree and type). This could potentially be improved in future studies by increasing the sample size and performing a longitudinal study, with more than one measurement per participant, to better highlight the directionality of EF performance as a potential consequence of HL. Despite selecting a limited number of subtests, the length of the test may have tired participants and eventually led to lower performance due to lack of interest, demotivation, and inattention. Although raw scores were converted according to the normative tables provided by the ENI-2, the lack of a control group limited the methodological quality of the study. Regarding the cognitive flexibility subtest, data from five participants were not considered for analysis due to their incomplete assessments, possibly influencing the statistical significance of our results.
In conclusion, participants showed performed better on attention and non-semantic graphic fluency subtests, while reporting more difficulties in visual memory domains, including both encoding and recall skills subtests. Nonetheless, our sample of Colombian children and adolescents with HL who were receiving multidisciplinary therapy achieved similar EF results to their normal hearing peers.