INTRODUCTION
Breast cancer is the most common type of cancer worldwide, with an estimated 2.3 million new cases annually. It is also the leading cause of cancer-related mortality among women, with approximately 666,103 deaths reported globally in 2024 (Ferlay et al., 2024; International Agency for Research on Cancer, 2024). In Brazil, breast cancer remains the most prevalent malignancy among women, with 73,610 new cases expected by 2025, a rate of 66.54 cases per 100,000 women, and approximately 18,000 annual deaths (National Cancer Institute, 2022).
Women diagnosed with breast cancer or undergoing treatment (such as surgery, chemotherapy, radiotherapy, or hormone therapy) face multiple challenges that go beyond the physical illness, including functional limitations, altered body image, and emotional stress. These factors can compromise self-esteem and negatively affect quality of life (Pierrisnard et al., 2018). The type of surgery (mastectomy or conservative) directly influences self-esteem, with lower scores being observed in women who undergo mastectomy (Joaquín-Mingorance et al., 2019). Moreover, side effects such as chemotherapy-induced alopecia and severe fatigue can affect emotional well-being and body image (Dunnill et al., 2018; Versluis et al., 2022).
Self-esteem, defined by Rosenberg (1965) as an individual’s overall evaluation of their own worth, plays a central role in coping with chronic illnesses such as breast cancer. In his work on self-esteem, Rosenberg emphasizes the importance of this construct in psychological adjustment, noting that individuals with higher self-esteem tend to display greater emotional resilience and adaptability when coping with stressors. The Transactional Model of Stress and Coping developed by Lazarus and Folkman (1984) reinforces this perspective by positing that self-esteem acts as a psychological resource that mediates emotional and behavioral responses to stressful situations, including chronic illness. Low self-esteem has been consistently associated with greater susceptibility to anxiety, depression, and diminished quality of life (Cortés & Justicia, 2008; Joaquín-Mingorance et al., 2019; Valverde et al., 2014).
Although the importance of self-esteem in the oncological context has been widely recognized, studies have reported conflicting findings. For example, an Iranian study with 261 women reported a high likelihood of low self-esteem (Yektatalab & Ghanbari, 2020), whereas an Indonesian study with 56 participants undergoing neoadjuvant chemotherapy found self-esteem levels within the normal range (Aprilianto et al., 2021). These inconsistencies suggest that sociodemographic, clinical, behavioral, and cultural factors may influence self-esteem outcomes. Few studies have comprehensively examined these dynamics in Brazil, a developing country with continental dimensions and significant regional disparities in income and healthcare access, where religiosity plays a key role (Ipsos Institute, 2023; Martins et al., 2021).
Understanding these associations is essential for developing comprehensive care strategies designed to mitigate damage to self-esteem and enhance well-being. This study therefore aimed to analyze the self-esteem of women with breast cancer undergoing oncological treatment and its association with sociodemographic, clinical, behavioral, and treatment-related variables.
METHOD
Study design
This is a quantitative, cross-sectional study with both descriptive and inferential analytical approaches. Descriptive statistics were employed to characterize the sample, while inferential techniques, specifically regression analysis, were used to examine associations between the variables of interest.
Participants
The study population consisted of women diagnosed with breast cancer at a High-Complexity Oncology Center in Brazil. The population included all women diagnosed with breast cancer at any stage of treatment at the institution in 2022, totaling 270 patients. The inclusion criteria were as follows: being aged 18 or older, having a confirmed breast cancer diagnosis, currently undergoing any form of oncological treatment (such as chemotherapy, radiotherapy, surgery, or hormonal therapy) at the Center, and the ability to understand and complete the data collection instruments. Women with a hearing, vision, speech, or cognitive impairment limiting their ability to answer or complete the data collection instruments were excluded. Participants were selected through direct contact by the researcher at the institution. At least two contact attempts and the implementation of inclusion and exclusion criteria yielded a final population of 210 women.
Measurements
Two instruments were used during data collection. Sociodemographic, behavioral, clinical, and treatment-related variables were assessed using a structured questionnaire developed by the research team based on a literature review. Content was validated by a panel of seven experts, researchers with PhDs with expertise in oncology and/or the development and validation of measurement instruments, who evaluated the items for clarity, coherence, presentation, and relevance. For analytical purposes, the following variables were dichotomized: age (≤ 49 vs. ≥ 50 years), race/ethnicity (White vs. non-White), municipality of residence (Muriaé vs. other), marital status (partnered vs. unpartnered), children (yes vs. no), type of employment (paid vs. unpaid), monthly household income (≤ 4000 vs. ≥ 4001 BRL), housing (owned vs. other), educational attainment (up to elementary school vs. high school and beyond), religious belief (yes vs. no), religious attendance (yes vs. no), engagement in religious practices (yes vs. no), alcohol use (yes vs. no), smoking (yes vs. no), illicit drug use (yes vs. no), physical activity (yes vs. no), presence of chronic illness (yes vs. no), daily use of continuous medications (yes vs. no), type of healthcare coverage (supplementary/private vs. public/Sistema Unica de Saúde (SUS)), time since cancer diagnosis (≤ 6 vs. ≥ 7 months), current cancer treatment (with vs. without chemotherapy), presence of symptoms or side effects (yes vs. no), number of treatment sessions (≤ 15 vs. ≥16), previous cancer treatment (yes vs. no), duration of current treatment (≤ 6 vs. ≥ 7 months), history of previous or concurrent cancers (yes vs. no), and presence of significant life events (yes vs. no).
The Rosenberg Self-Esteem Scale (RSES), originally developed by Rosenberg in 1965 and adapted to Portuguese by Dini et al. (2004), was used to assess self-esteem. The instrument consists of 10 items rated on a 4-point Likert scale (ranging from 1 = “strongly disagree” to 4 = “strongly agree”), with five items assessing positive self-image and five assessing negative self-image. Total scores range from 10 to 40, with higher scores indicating greater self-esteem. Scores were classified as low (< 20), average (20–30), or high (> 30). For analytical purposes, self-esteem was dichotomized into high (> 30) and average/low (≤ 30). The RSES has shown acceptable internal consistency, with Cronbach’s alpha values ranging from .71 to .87 in previous studies (Bano et al., 2022; Tsai et al., 2021).
Procedure
Data collection was conducted between November 2022 and February 2023 at the hospital. Participants were approached individually in each area of treatment (chemotherapy, radiotherapy, hormone therapy, and surgery) at the oncology service. To avoid interruptions, interviews were conducted before or after the scheduled treatment sessions. This approach ensured that data collection did not interfere with the treatment routine or cause disruptions for either the patients or healthcare professionals. Data were collected through individual interviews lasting approximately 20 minutes, during which two instruments were administered (the Sociodemographic and Clinical Questionnaire and the Rosenberg Self-Esteem Scale). The researchers completed the instruments based on participants’ responses, ensuring uniformity. In cases where participants had difficulty understanding the questions, the researchers repeated them slowly, as often as necessary, without altering the content or providing synonyms. This ensured that the reading was consistent and no interpretation was made of the questions, preventing any bias in responses. Due to the COVID-19 pandemic, all health measures were observed, including mask usage, social distancing, and surface disinfection with 70% alcohol.
Statistical analysis
The data were double-entered for quality control and analyzed using IBM SPSS Statistics 24.0. Descriptive statistics (frequencies, percentages, means, and standard deviations) were calculated. Pearson’s Chi-square and Fisher’s Exact tests were used to assess associations between self-esteem levels and independent variables. The internal consistency of the RSES was assessed using Cronbach’s alpha coefficient, with values ≥ .70 being considered acceptable. The dependent variable for the logistic regression was self-esteem, dichotomized as high self-esteem (scores > 30) and average/low self-esteem (scores ≤ 30), based on the cut-off points established in the Rosenberg Self-Esteem Scale. All 27 independent variables were included in the model. The final model was constructed using the Forward Stepwise selection method, and variables that failed to meet the significance criteria (p < .05) were not retained in the final model. Model adequacy was assessed using the -2 Log Likelihood, Cox & Snell R2, Nagelkerke R2, and the Hosmer-Lemeshow goodness-of-fit test to confirm the model fit with the observed data, ensuring the reliability and validity of the regression results.
Ethical considerations
The study was approved by the Research Ethics Committee of a Brazilian public university with protocol No. 5,688,277.
RESULTS
The sociodemographic profile of the 210 participants revealed that 51.4% were aged between 50 and 69. Regarding race/ethnicity, 42.4% identified as white and 41.4% as mixed race. Most participants resided in municipalities outside the study location (88.1%), including regions in the states of Minas Gerais, Rio de Janeiro, Espírito Santo, and the Federal District. In terms of marital status, 59.5% were partnered, while 33.8% had two and 31.9% had three or more children.
Regarding employment, participants displayed similar proportions of unemployment (29.0%), sick leave (29.0%), and retirement (28.2%). The majority reported a household income of up to one and a half minimum wages (57.6%) and lived in their own homes (70.0%). In terms of educational attainment, most participants had incomplete elementary education (44.3%). Religiosity was significant, with 96.1% professing a religion and 90.0% attending religious institutions.
As for the breast cancer diagnosis, 49.5% had been diagnosed between seven and 24 months earlier, and 51.0% were undergoing chemotherapy. Most participants had already undergone more than 15 treatment sessions (67.6%), and 44.3% had been in follow-up care for seven to 24 months. A total of 18.1% reported metastasis, with the bones (28.3%) and lungs (18.9%) being the most frequent sites.
In regard to significant life events, 66.6% of participants reported having experienced at least one. Seventy per cent cited a single event, the most common one being the cancer diagnosis (49.3%), followed by the loss of a loved one (40.0%). Positive events, such as the birth of children or grandchildren and new friendships, were mentioned by 13.6%.
Table 1 shows the distribution of the women by their responses to the items in the Rosenberg Self-Esteem Scale.

The distribution of women undergoing oncological treatment for breast cancer was analyzed separately based on their responses to the statements in the Rosenberg Self-Esteem Scale, as shown in Table 1. They were classified according to their responses to statements evaluating positive (1, 3, 4, 7, and 10) and negative feelings (2, 5, 6, 8, and 9).
Regarding the positive feelings statements (1, 3, 4, 7, and 10), the majority of respondents strongly agreed (score 4), with percentages ranging from 73.3% (154) to 89.6% (188). These statements displayed scores ranging from three to four, the highest on the scale for these items, reflecting participants’ high self-esteem.
For the negative feelings statements (2, 5, 6, 8, and 9), most participants strongly disagreed (score 4), with percentages ranging from 61.4% (129) to 87.6% (184). It was also observed that scores were high for these statements. Statements 6 (“At times, I feel useless”) and 8 (“I wish I could have more respect for myself”) showed significant percentages of women with breast cancer reporting a score of 1 (strongly agree), 11.4% (24) and 19.5% (41), and a score of 2 (agree), 22.9% (48) and 13.3% (28), respectively. These are the lowest scores on the scale (Table 1).
Table 2 presents the distribution of women with breast cancer undergoing oncological treatment by self-esteem classification.
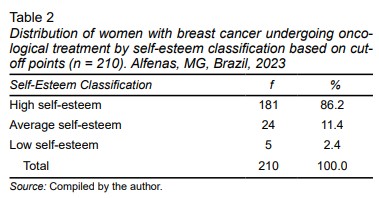
An analysis of the distribution of women with breast cancer by self-esteem classification based on the cutoff points showed that 86.2% (181) of respondents were classified as having high self-esteem. Additionally, 11.4% (35) were classified as having average self-esteem, while 2.4% (five) were classified as having low self-esteem (Table 2).
The internal consistency of the Rosenberg Self-Esteem Scale was assessed using Cronbach’s alpha coefficient, yielding a value of .835. The analysis indicated that the items evaluated demonstrated homogeneity and adequate correlation, making the internal consistency of the instrument acceptable for this study. This finding supports the reliability of the scale in assessing participants’ self-esteem.
In the univariate analysis, no significant associations were found between self-esteem and sociodemographic variables such as age group, race/ethnicity, municipality of residence, marital status, number of children, and employment status. Likewise, no significant associations were found between lifestyle habits, including alcohol consumption, smoking, illicit drug use, physical activity, and the presence of chronic diseases. No association was found between participants’ self-esteem and clinical factors, such as continuous medication use, type of care, time since cancer diagnosis, and type of current treatment, as well as treatment-related variables, such as the number of sessions, previous treatments, treatment duration, and the presence of prior or concomitant cancers (p > .05).
However, associations with self-esteem were identified for the following variables: religious beliefs, habits related to religiosity, symptom(s)/side effect(s), and significant life events, as shown in Table 3.
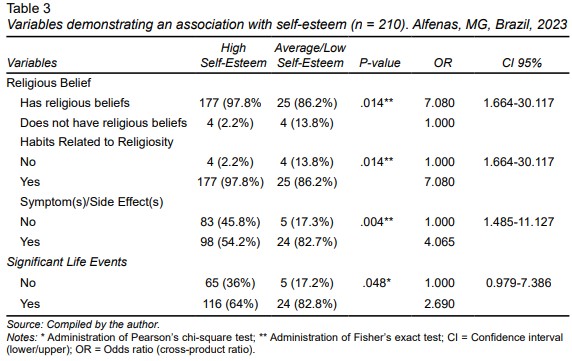
The analyses revealed a significant association with the “religious belief” (p = .014) and “habits related to religiosity” (p = .014) variables, showing that women with religious beliefs and religious habits are approximately seven times more likely to have low or average self-esteem. Similarly, the “symptom(s)/side effect(s)” (p = .004) variable showed that participants reporting these symptoms are about four times more likely to have low or average self-esteem. Finally, the “significant life events” (p = .048) variable indicated that women who had experienced significant life events were twice as likely to have low or average self-esteem.
Table 4 presents the evaluation of the logistic regression model parameters for the independent variables with self-esteem. After analyzing the parameters of all the independent variables influencing self-esteem using the logistic regression model, it was found that the “religious belief” (p = .017), “habits related to religiosity” (p = .001), “presence of symptom(s)/side effect(s)” (p = .005), and “significant life event” (p =.030) variables showed significant associations, resulting in a final adjusted model (Table 4).
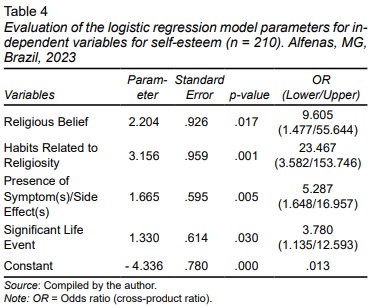
The model revealed that women with breast cancer undergoing oncological treatment who hold religious beliefs are approximately nine times more likely to have low or average self-esteem. Moreover, participants with habits related to religiosity were approximately 23 times more likely to develop low or average self-esteem. Regarding the presence of symptom(s)/side effect(s), the model indicates that the likelihood of having low or average self-esteem is approximately five times higher than in women without symptoms/side effects. Finally, it was observed that women who had experienced a significant life event were about three times more likely to have low or average self-esteem (Table 4).
In addition to the interpretation of model coefficients, the adequacy of the logistic regression model was assessed using statistical fit indices. The -2 Log Likelihood progressively decreased during the selection process, achieving a final value of 137.131 in Step 4, indicating improvements in model fit with each step. Cox & Snell R2 and Nagelkerke R² values showed that the final model explained 13.9% and 25.2% of the variance in self-esteem classification respectively. Furthermore, the Hosmer-Lemeshow goodness-of-fit test did not indicate a significant lack of fit (χ² = 1.448; p = .919), suggesting a good model fit for observed data.
DISCUSSION AND CONCLUSION
The analysis of the sociodemographic profile highlighted relevant characteristics aligned with the literature, such as the predominance of women aged between 50 and 69, the age group when breast cancer is most frequent (Andrade et al., 2023). Most participants were white or mixed race, reflecting Brazil’s demographics (Brazilian Institute of Geography and Statistics, 2022), and resided in municipalities outside the treatment location, underscoring the need for oncological care decentralization (Andrade et al., 2023).
The presence of a partner, observed in 59.5% of participants, may contribute to emotional stability and well-being during treatment, as suggested by previous literature (Bastianello & Hutz, 2016). However, the low family income and limited educational attainment observed in a large proportion of participants highlight economic and educational vulnerabilities requiring specific health intervention strategies (Gratão et al., 2023).
The analysis of the distribution of women with breast cancer undergoing oncological treatment using the Rosenberg Self-Esteem Scale showed that most displayed high percentages (above 73.3%) of agreement with statements reflecting positive feelings, such as self-acceptance, self-appreciation, and self-confidence. These feelings reflect a positive self-view and belief in their abilities (Branden, 2000; Kernis, 1995).
However, the impact of these feelings on women with breast cancer is modest, given the emotional, physical, and social challenges of the disease affecting their psychological well-being (Almeida et al., 2012; Kim et al., 2021). Medical procedures and physical changes can undermine self-acceptance and self-confidence (Almeida et al., 2012; Hagen et al., 2021). Additionally, these women face stigma, isolation, and pressure to maintain a positive image, which may negatively impact their self-esteem (Yektatalab & Ghanbari, 2020).
Recognizing these complex experiences and providing support from the multidisciplinary team with interventions designed to strengthen emotional and social well-being is essential for helping women cope with the challenges of breast cancer diagnosis and treatment (Iddrisu et al., 2020; Adib-Hajbaghery et al., 2021).
Religiosity was widely reported, with 96.1% of participants professing a belief. Faith can act as emotional support but also revealed unexpected associations with average or low self-esteem, suggesting that factors such as religious guilt and social pressures may play a role (Gall & Bilodeau, 2020; Esperandio et al., 2022). This ambivalence has been widely documented in the literature (Koenig, 2012; Leal et al., 2022; Pargament, 2007).
While religiosity is often seen as a coping resource that offers emotional comfort and a sense of purpose (Koenig, 2012; Pargament, 2007), Pargament’s theory of religious coping shows that in certain contexts, it can also contribute to spiritual struggles. When individuals interpret illness as divine punishment or experience feelings of religious inadequacy, religiosity can increase rather than alleviate emotional distress (Pargamentet al., 1998).
This dynamic may explain why variables such as “religious belief” and “habits related to religiosity” showed significant associations with lower self-esteem in this study. While religiosity is often seen as a source of emotional support, some women reported feelings of guilt or frustration when their religious practices failed to provide the expected healing or relief, which may have negatively impacted their self-esteem (Mkuu et al., 2021). These findings underscore the importance of not only recognizing the presence of religiosity but also of understanding how patients internalize and relate to their faith during illness.
Furthermore, religious environments can serve as spaces for social comparison, where women with breast cancer feel unworthy or less spiritually favored. This sense of spiritual abandonment can intensify frustration and insecurity, resulting in lower self-esteem (Ferreira et al., 2020; Esperandio et al., 2022).
The “symptom(s)/side effect(s)” variable also demonstrated a significant association with self-esteem. Physical changes resulting from treatment, such as alopecia, radiodermatitis, and lymphedema, can negatively affect self-image and contribute to low self-esteem due to the perception of loss of attractiveness (Almeida et al., 2012; Kim et al., 2021). According to the Transactional Model of Stress and Coping (Lazarus & Folkman, 1984), these physical symptoms are primary stressors patients appraise in terms of their impact on personal identity and daily functioning.
When symptoms challenge bodily integrity, an essential component of self-concept, especially for women, this can result in heightened psychological vulnerability. Side effects such as fatigue, musculoskeletal pain, and gastrointestinal disorders hinder daily activities and impose dietary restrictions, perceived as limitations affecting self-image and self-esteem. The persistence of these side effects reinforces feelings of inadequacy, worthlessness, and social withdrawal, further exacerbating psychological distress (Keaver et al., 2021; Kruif et al., 2021).
“Significant life events” showed a significant association with self-esteem, particularly the cancer diagnosis, which can be perceived as a traumatic event. The uncertainty and emotional impact associated with the diagnosis can undermine self-esteem and increase emotional vulnerability (Almeida et al., 2012). This observation is consistent with the stress proliferation theory (Pearlin et al., 1981) positing that major life events often trigger secondary stressors that accumulate and amplify emotional distress.
For example, women undergoing cancer treatment may simultaneously have to deal with personal loss, financial strain, and family disruptions, compounding the psychological burden. Conversely, positive life events, such as the birth of a grandchild, may act as protective factors that buffer the negative impact of illness and positively influence self-esteem, highlighting the importance of support networks in coping with the disease (Iddrisu et al., 2020; Hagen et al., 2021).
The internal consistency of the Rosenberg Self-Esteem Scale was satisfactory in the present study (α = .835), indicating its reliability for assessing self-esteem. Comparative international studies revealed similar coefficients, reinforcing the robustness of the scale across cultural contexts (Yektatalab & Ghanbari, 2020; Bano et al., 2022).
The findings related to religiosity should be interpreted in light of the Brazilian sociocultural context, where religious beliefs and practices are deeply rooted in daily life and often serve as key coping mechanisms in situations of illness and suffering. A global survey conducted by the Ipsos Institute (2023) in 26 countries found that Brazil, together with South Africa, has the highest proportion of people believing in God or a higher power (89%). Among Brazilians, 76% reported praying outside a place of worship (for example, at home), while 49% reported regularly attending religious services. Paradoxically, the results of this study revealed that both holding religious beliefs and engaging in habits linked to religiosity were associated with lower self-esteem in women undergoing oncological treatment.
This may reflect internal spiritual conflict, guilt, or the perception of illness as divine punishment, patterns that have been observed in other Brazilian populations coping with chronic illness (Borges et al., 2022; Leal et al., 2022). Moreover, the association between lower self-esteem and the presence of symptoms or side effects, as well as recent significant life events, highlights the multidimensional burden these women face. In a country marked by social inequality, limited access to specialized psychosocial support, and strong family and religious structures, these findings underscore the need for culturally sensitive care approaches that not only consider clinical but also emotional and spiritual dimensions of the experience of illness. It is therefore essential for healthcare teams to be trained in recognizing and addressing spiritual struggles as part of holistic oncological care, to ensure that religious beliefs serve as a source of comfort rather than an additional source of distress (Branco & Silva, 2017; Dias & Pais-Ribeiro, 2019).
This study has significant limitations that must be considered. Its observational nature prevents the inference of causality between the variables analyzed and self-esteem, while the sample size (210 women) and refusals to participate may limit the generalizability of findings and introduce potential selection bias. Additionally, the subjectivity inherent to the construct evaluated may have resulted in different interpretations by participants, influencing their responses.
To overcome these limitations, future studies should adopt prospective designs with nationally representative samples, enabling the evaluation of causal relationships and the identification of modifiable associated factors. It is also necessary to explore interventions such as educational practices and psychological support to promote and sustain self-esteem in women with breast cancer.
This study found that most women with breast cancer undergoing oncological treatment display high levels of self-esteem, despite the challenges posed by the disease. However, variables such as religious beliefs, habits related to religiosity, symptoms/side effects, and significant life events showed significant associations with self-esteem. These factors often negatively affect patients’ self-perception, emphasizing the need for special attention to emotional, social, and spiritual aspects during oncological care.
Caring for the self-esteem of women with breast cancer requires an integrated approach by healthcare professionals. Beyond clinical care, it is essential to provide emotional support, establish empathetic connections, clarify doubts about treatment, and address patient concerns. Individualized, comprehensive care aids in adapting to physical and emotional changes, contributing to building self-esteem. Based on the findings of this study, it is crucial for the multidisciplinary team to be aware of the importance of delivering holistic care, improving patient/family/professional/institution interaction, and fostering more effective coping with the disease.